
1) Assesment before IVF
This is a vital stage which sometimes tends to be ignored. Many of the couples referred to IVF, may possibly benefit from other treatment.
Before we commence actual IVF, we run a number of tests, as sperm counts, blood and hormone tests to confirm that you have a chance of success.
We tailor your treatment to suit your individual needs. We also try, when feasible, to offer effective (alternative) treatments before we embark on IVF.
2) Ovarian stimulation and monitoring
The best chance of successful pregnancy is usually obtained when more than one embryo is placed in the uterus during embryo transfer. This is because so many early hyman embryos, normally fertilised, are lost normally or do not develop into a baby. One way of overcoming this is to put two embryos back at once during IVF. When two or three embryos are put back together the risk of a multiple pregnancy is not necessarily as great as you might expect, though it is certainly higher than in natural conception.
In order to obtain more than one embryo simultaneously, we obviously need more than one egg. This is why drugs are given to make the ovaries work harder than normally. Occasionally many eggs are obtained simultaneously with these drugs and many of them fertilize and make an embryo.
Drugs, either pills or injections to make you ovulate, will normally be given to you a few days after your period, at the start of the treatment cycle. We vary the dose and the length of time these drugs are given, depending on your individual responce. This usually results in the ovaries responding more effectively to the treatment. More eggs seem to be produced, with a higher pregnancy rate in certain cases. The doctor co-ordinating your treatment will explain this fully.

We time egg collection to within two or three hours of when we expect you to ovulate. If eggs are not collected fairly close to this time they may not fertilize properly. This is why we invest in so many tests to confirm the progress of your hormone results and the development of your eggs.
Each egg grows in a fluid-filled follicle (a small balloon-like structure) in the ovary. The follicle grows in size during the first few days after your period. Normally, ovulation (when an egg escapes from its follicle) occurs when the follicle is just under one inch across – usually around the twelfth to fourteenth day of your cycle.
There are basically three ways by which we try to make sure that we collect mature eggs. None is wholly accurate and a good deal of experience is used to pinpoint the moment before ovulation. There are two tests and a drug treatment.
Hormone tests: During IVF treatment, the hormones oestrogen and progesterone are produced in increasing amounts. Regular blood tests ( usually tests of oestrogen levels ) detect the increase
Firstly, measurement of oestrogen can help predict whether or not the ovaries are responding sufficiently well to justify proceeding to the next stage, egg collection. This is particularly helpful in some difficult cases, particulary those women who do not respond well to stimulation of the ovaries. We would obviously prefer to abandon egg collection if there is no chance of pregnancy, rather than cause patients unnecessary distress, and the extra expense of a complete (albeit destined to fail) IVF treatment cycle.
Secondly, oestrogen measurerement may give an indication that the ovaries are responding to the fertility drugs too vigorously. This early sign seems to be helpful sometimes in avoiding some of the more serious complications of ovarian over-stimulation.
Thirdly, and often most important, the results of hormone tests are very useful indeed when trying to decide after the event why a particular treatment cycle has failed, and sometimes whether or not a repeated treatment cycle is realy worthwhile. This alone seems to us to be the key reason why we continue to put patients to the added inconvenience of repeated blood tests, and to justify the extra money they have to spend.
Ultrasound: the swelling follicle can be directly measured using ultrasound. Ultrasound works like a ship-sonar, used to detect objects under sea-water. In this case the object being detected is the ovary containing the follicle and the “sea-water” is either urine in the bladder or the body fat, which is almost liquid! Ultrasound is usually done daily – we know from experience that when the follicle is about 20 millimeters across, ovulation is fairly imminent. In recent years, ultrasound has become more and more accurate and sophisticated, and our machines are regularly upgraded in order with the advancing technology.
Ultrasound measurements are also indirectly useful in timing egg collection because with ultrasound we can assess the thickness of the uterine lining – the endometrium. A reasonably thick endometrium tends to argue that the uterus is fairly “ripe” and will be shortly ready to receive an egg or an embryo.
One further way of ensuring that we collect mature eggs is by giving an injection of hCG shortly before we expect ovulation. This drug is very similar to your own luteinising hormone and can give a message to the ovary to ovulate.
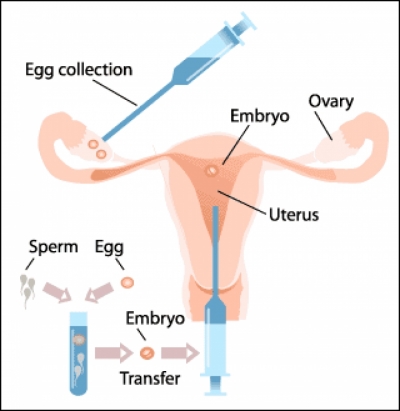
3) Egg Collection
When ovulation is about to occur, the laboratory team is mobilised. The eggs will be collected under ultrasound guidance (usually under sedation).
4) Fertilization
The eggs collected are incubated in the culture medium, which contains very precisely measured amounts of nutrients needed for the egg’s survival.
Before the egg is incubated, usually shortly before egg collection, we ask the husband to produce semen by masturbation. The semen is taken to the laboratory. In the laboratory, the sperm are washed and diluted and the number of sperm counted under a microscope. Several hours after egg collection, spermatozoa will be mixed with the fluid containing the egg. Hopefully, fertilization will take place within a few hours. It is not uncommon to find a problem with the sperm – which may be too few in number or too weak in other ways. At present we need several thousand normal sperm for standard/conditional/routine IVF otherwhise we proceed to sperm micro injection (ICSI).
5) Embryo culture and Embryo transfer
A cultured egg is usually inspected under the microscope at 18 hours after placing it with sperm, and then again about 30 hours later. The inspection at 18 hours is important, because this is a milestone time when usually the first signs of normal fertilisation can be observed. Normally the embryo will have divided into two or four cells in 48 hours, although occasionally growth may be somewhat more advanced. Before an embryo is transferred back to the womb, we make sure it appears normal. If there is doubt about this we may wait a further 24 hours before taking a decision whether we should transfer it or not (With current scientific evidence it is not detrimental to the outcome if embryo transfer takes place on day 2 or 3 after fertilization). Our team is curretly researching the hypothesis that a late transfer on day 4 or 5 after fertilization may offer the benefit of choosing the best embryo.
Embryos that seem seriously abnormal are not transferred. They are either discarded if that is the couple’s wish, or alternatively studied to see if we can find out why they grew abnormally.
6) Blastocyst transfer
See more about the blastocyst transfer.
