
Preimplantation Diagnosis
(Infographic: http://www.ivf-worldwide.com/cogen/oep/121-pgd-pgs.html)
What is Preimplantation Genetic Diagnosis (PGD)?
PGD is a technique that enables couples with an inheritable condition in their family to avoid passing it on to their children. The process helps potential parents prevent the birth of a child with a serious genetic condition.
PGD is used when one or both parents have a known genetic abnormality. It involves checking the genes and/or chromosomes of embryos created through IVF to determine if it has also inherited the abnormality.
PGD involves the use of assisted reproductive technology (ART). Eggs are obtained and fertilised through in vitro fertilisation (IVF). Once fertilised, the embryos develop for 2-3 days and then cells are removed from each embryo. The genetic material (DNA or chromosomes) within one cell of the embryo is then tested for the genetic or chromosomal abnormality. Up to two unaffected embryos are then transferred to the woman’s uterus to implant.
If successful, the procedure will result in pregnancy and the child should not be affected by the condition for which it was tested.
Who is PGD for?
PGD may be recommended for:
- Carriers of a serious autosomal recessive condition:
For carriers of an autosomal recessive condition, there is a 1 in 4 (25%) risk of each pregnancy delivering an affected child.
- Carriers of a serious autosomal dominant condition: For carriers of an autosomal dominant condition, there is a 1 in 2 (50%) risk of each pregnancy delivering an affected child.
- Couples with chromosome disorders.
- Couples with a family history of serious sex-linked disorders: Couples with a family history of a sex-linked disorder have a 1 in 4 (25%) risk of each pregnancy delivering an affected child (half of all male children).
What conditions can be diagnosed using PGD?
PGD can be used to test for virtually any genetic condition where a specific gene is known to cause that condition. It is currently approved to screen for over 250 genetic conditions.
PGD is available for three broad categories of conditions including:
- Single gene defects for which PGD testing is available.
- Chromosomal abnormalities, including inversions, deletions, aneuploidy (an abnormal number of chromosomes), and translocations (where a piece of one chromosome either becomes attached to another chromosome or swaps places with a segment from another chromosome).
- Sex-linked conditions for which it is not yet possible to test for the specific genetic mutation.
What are the risks of PGD?
With PGD, there is also the possibility that:
- some embryos may be damaged by the process of cell removal
- testing may not be 100% reliable or conclusive.
How does PGD work?
The typical treatment cycle for PGD is as follows:
Step 1: Stimulation of the ovaries
In order to create embryos for genetic testing, the ovaries have to be artificially stimulated using hormones to produce several eggs at one time.
Because a significant number of a couple’s embryos are likely to be affected by the genetic or chromosomal abnormality, a large number of embryos need to be created for the best chances of success.
Step 2: Collection of eggs from the ovaries
At the appropriate time, the eggs are removed in a process known as egg retrieval. Once the eggs are removed, they are inspected to determine which are mature and normal appearing.
Step 3: Insemination/injection of sperm
Fertilisation during PGD will be done either by:
- In Vitro Fertilisation (IVF): Sperm and eggs are placed together in a culture dish to allow fertilisation to occur. This technique is used mainly for chromosome abnormalities or sex-linked conditions.
- Intracytoplasmic Sperm Injection (ICSI): Single sperm is injected in the centre of an egg. This technique is used for conditions caused by a single faulty gene.
Step 4: Fertilisation
The morning after injection/insemination of the sperm, the embryologist carefully examines each egg to see if fertilisation has occurred.
Step 5: Embryo biopsy
The eggs that were successfully fertilised are grown in the laboratory for 2-3 days until the cells have divided and the embryo consists of around 8 cells. An embryologist removes one or two of the cells (blastomeres) from the embryo.
This technique is highly specialised and can only be carried out by embryologists who have a special licence from the Human Fertilisation and Embryology Authority (HFEA).
The removal of these cells should not harm the embryo.
Trophectoderm biopsy
Instead of removing and testing one or two cells from a 2-3 day old embryo, clinics may allow the embryo to develop for 5-6 days, when there are 100-150 cells. Because more cells can be removed at this stage from the trophectoderm (the cells which will form the placenta), this type of biopsy could possibly lead to a more accurate diagnostic test.
Step 6: Embryo Testing
The cells are tested to see if the embryo from which they were removed contains the abnormality that causes the genetic condition in the family.
Step 7: Embryo Transfer
Only those embryos that do not have the specific genetic condition that was tested for will be transplanted into the woman’s uterus. No more than two embryos will be transferred to the uterus at any one time to avoid the possibility of multiple births (more than one baby in a pregnancy).
Any suitable remaining unaffected embryos can be frozen for later use.
Those embryos that are affected by the inherited condition are allowed to perish.
Step 8: Pregnancy Test
About two weeks after the embryo transfer, the woman is given a pregnancy test. A positive pregnancy test means that at least one embryo has implanted.
Sex selection
Some genetic diseases only affect one sex rather than the other. Examples include Duchenne muscular dystrophy, which affects boys but not girls. (Girls may still ‘carry’ the gene for the disease but they will not suffer from it). In these sorts of cases, the embryo is tested to find out its sex and only embryos of the non-affected sex are transferred to the womb. In the UK, sex selection is only allowed to avoid having a child with a serious medical condition; it is illegal to carry out sex selection for social reasons (e.g. for family ‘balancing’).
What are the advantages of PGD?
For many genetic conditions, cures do not currently exist and are not likely to be found soon. Available treatments often carry substantial risks or have adverse effects. Even if effective, the psychological impact of late onset conditions on those at risk and on their families is significant. Therefore, the option of preventing the condition may be preferable to waiting for a possible cure to eventually become available.
PGD also provides:
- An alternative to prenatal diagnostic testing: Couplesavoid the distress associated with diagnosis, particularly if late in an established pregnancy, as well as the risk of miscarriage associated with such testing.
- An alternative to termination of pregnancy: If prenatal testing (through amniocentesis or chorionic villus tests) reveals a genetic abnormality, the options available to parents are to have a child with a genetic condition or to undergo a pregnancy termination. This is a difficult and often traumatic decision. However, PGD is performed before pregnancy begins, thus eliminating these difficult decisions.
- The opportunity to conceive a pregnancy that is biologically the parents’ own and yet unaffected by a genetic condition in the family:Couples for whom the option of prenatal testing and termination is not an acceptable choice are unlikely to want to take the risk of a child having a genetic condition. In the past, potential parents with a genetic condition or those who know that they are carriers frequently chose adoption, embryo donation, or surrogacy or chose not to have children in order to avoid the risk of passing on the condition. PGD now allows these couples the opportunity to have a child free of the condition.
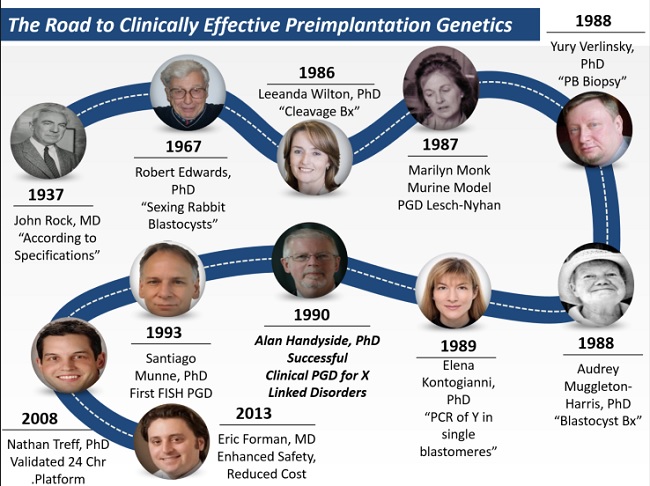
The first PGD clinical cases
I had the honor to perform the genetic analysis for the first PGD cases worldwide while I was studying for my PhD at the Hammersmith Hospital. In the team of Professor Lord Robert Winston and Professor Alan Handyside I was developing single-cell PCR for diagnosing genetic diseases.
The approach that was used for the world’s first PGD cases was identifying the sex of the embryo and transferring only female embryos in the uterus in order to avoid sex-linked genetic diseases.
Female embryos were selectively transferred in five couples at risk of X-linked disease, resulting in two twins and one singleton pregnancy. Because the Y chromosome region I was amplifying contained many repeats, it was more efficient than trying to amplify a unique region.

A band on the PCR gel indicated that the embryo was male and the absence of a band indicated that the embryo was female. However, amplification failure or an anucleate blastomere also resulted in absence of a band on the PCR gel. To reduce the risk of misdiagnosis I went on to co-amplify sequences on the X and Y. At that time nothing was known about allele dropout, cumulus cell contamination, or amplification failure from single cells. During the 1980s, human IVF embryos were exclusively transferred on day two of development as the culture medium used was incapable of reliably growing embryos past this stage.
Since the biopsy was to be performed on day three, the first diagnoses were all performed in one day, with transfer of the embryos late on day three. A comparison of day two and day three transfers indicated that this would not adversely affect pregnancy rates.
The worry of embryos arresting was so high that some transfers took place in the early hours of day four so that the embryos were removed from culture as soon as possible. There were many evenings at the Hammersmith when a transfer was performed at 1 a.m. on day four and we returned to the laboratory at 7 a.m. to start the next case. Prof. Winston helped deliver most of the first PGD babies.
After the first clinical cases at Hammersmith Hospital, thousands of babies were born after PGD. It is still the main method of preventing a pregnancy with an embryo carrying an inherited genetic disease.
References:
http://www.nature.com/nature/journal/v344/n6268/abs/344768a0.html
http://assets.cambridge.org/97805218/84716/excerpt/9780521884716_excerpt.pdf
http://www.mayoclinic.org/tests-procedures/genetic-testing/basics/definition/prc-20014802
http://www.geneticalliance.org.uk/aboutpgd.htm
